 The July issue of Acta Paediatrica offers a collection of free, live links to a volley of rebuttals published over the past four months to an article in March submitted by medical ethicist Dr. Niels Lynøe and most of the other experts who informed the 2016 Swedish report critical of shaking theory, commissioned by an independent agency in Sweden whose name is abbreviated SBU.
The July issue of Acta Paediatrica offers a collection of free, live links to a volley of rebuttals published over the past four months to an article in March submitted by medical ethicist Dr. Niels Lynøe and most of the other experts who informed the 2016 Swedish report critical of shaking theory, commissioned by an independent agency in Sweden whose name is abbreviated SBU.
In an email exchange last week, Dr. Lynøe wrote that his team knew the topic was controversial, but they were “rather surprised” at the vehemence of the criticisms. “I also think that there was something positive with the critical comments,” he added, “because we got the opportunity to explain and explore some aspects more.”

Dr. Niels Lynøe
The March paper reported on the same research as the SBU study, an exhaustive evaluation of the shaken baby literature that ultimately declared the scientific evidence behind shaking theory “weak.” The analysis noted fundamental problems with the bulk of the published research—in a typical study design, the report noted, researchers had applied the criteria they were attempting to prove when identifying and sorting their subjects, so the results necessarily supported their theory.
 Weeks after the Lynøe et al. paper appeared, Acta Paediatrica published an editorial by epidemiology professor Jonas F. Ludvigsson criticizing the SBU’s methods and warning of an “imminent risk” that the paper will discourage the reporting of child abuse and leave abused children undiagnosed. Dr. Ludvigsson conceded quality problems with past SBS research, but rejected the SBU’s conclusions and endorsed reliance on the triad:
Weeks after the Lynøe et al. paper appeared, Acta Paediatrica published an editorial by epidemiology professor Jonas F. Ludvigsson criticizing the SBU’s methods and warning of an “imminent risk” that the paper will discourage the reporting of child abuse and leave abused children undiagnosed. Dr. Ludvigsson conceded quality problems with past SBS research, but rejected the SBU’s conclusions and endorsed reliance on the triad:
“[The study’s] publication in Acta Paediatrica does not spell the end of the discussion. Instead, it is a clear signal that more research is needed. But for now, paediatricians should continue to alert social services when they observe a child with the triad, once other explanations for subdural haematomas, retinal haemorrhages and brain ischaemia and oedema have been ruled out.”
The next critique of Lynøe et al., in mid April, added irony to the collection by denying the triad itself. An editorial by violence and abuse specialist Dr. Steven Lucas and others charged that the SBU’s methods had become “untethered from the agency’s published methodology” and argued that the study was fundamentally flawed, because it had examined the question of whether the presence of the triad proves infant shaking. Lucas et al. wrote:
“The construct of the ‘triad’ represents a rhetorical fallacy known as a straw man, which gives the impression of refuting an opponent’s argument – the ‘triad’ is pathognomonic for AHT – when, in fact, that argument was never advanced by that opponent. We maintain that the term ‘triad’ carries no value for clinicians experienced in evaluating suspected AHT.”

In refutation of the straw man argument, I point out that both Joshua Burns and Michelle Heale were convicted based only on the opinion of child abuse experts that the triad proves abusive head trauma—these cases are not unique, only easy to reference here. I myself have researched dozens of convictions based on the triad, sometimes on only one or two elements of the triad.
Lynøe et al. addressed the straw man argument in a response to a different criticism (the response to Narang et al.), by quoting these physician guidelines, which clearly endorse the triad:
“If there is no history of traffic accident or fall from a considerable height, the combination of subdural hematoma and encephalopathy with edema or hemorrhage strongly suggest that the infant has been abused. If there are also retinal hemorrhages then from the medical point of view the diagnosis of abuse is quite clear.”
 Also in April, Acta Paediatrica published an editorial by pediatric ophthalmologist Dr. Alex Levin, who declared, “There is a plethora of scientific evidence that retinal hemorrhages are a cardinal feature of abusive head trauma.” Among other objections to the study, he criticized the SBU’s failure to consider the various possible sizes and locations of retinal hemorrhages. “To ignore these descriptors,” he wrote, “is like saying that a rose is no different than any other ‘flower.'”
Also in April, Acta Paediatrica published an editorial by pediatric ophthalmologist Dr. Alex Levin, who declared, “There is a plethora of scientific evidence that retinal hemorrhages are a cardinal feature of abusive head trauma.” Among other objections to the study, he criticized the SBU’s failure to consider the various possible sizes and locations of retinal hemorrhages. “To ignore these descriptors,” he wrote, “is like saying that a rose is no different than any other ‘flower.'”
Dr. Levin also objected that the SBU team had ignored the “wealth of clinical experience” available from the community of child abuse experts. He argued that certain retinal findings, even in the absence of any other evidence, should shift the assumption to one of abuse:
“A diagnosis of abuse should not be made solely based on retinal haemorrhages, but certain retinal findings make that likelihood dramatically high, so high that one must actively seek (or rule out) supportive evidence that the child has been abused and is in need of protection.”
Another commentary in the April issue, by eye and vision specialist Dr. Kerstin Hellgren and others, called the SBU report “misleading.” In an apparent endorsement of both the triad and the literature that supports it, the authors wrote:
“The SBU report concludes that there is only limited evidence that shaking of an infant can cause the triad signs, in contrast with the numerous reports describing such lesions in victims of verified shaking. It is unfortunate that the SBU panel neither included a paediatrician nor a paediatric ophthalmologist with experience of child abuse to facilitate a correct interpretation of the cited papers.”
In a response to both Levin and Hellgren et al., the Lynøe authors reiterated their commitment to objectivity:
“If physicians involved in child protection teams embraced the research question as if it was a generally accepted scientific fact when classifying cases and controls, this would have resulted in circular reasoning when estimating the diagnostic accuracy of the triad. For that reason, and in order to avoid conflicts of interest and circular reasoning, the expert panel did not include any experts associated with child protection teams. The panel comprised two paediatricians and one expert each from the fields of forensic medicine, radiology, epidemiology and medical ethics. All the included had long experience of assessing scientific work and were scrutinised for potential conflicts of interest and cleared by the Agency. The expert panel followed the guidance in handbooks for assessing health technology and any other panel reproducing the study would have probably arrived at the same conclusions.”
In May, Dr. Sandeep Narang and Dr. Christopher Greeley, both renowned child abuse specialists, published a column in the Acta Paeditrica series “A Different View” that lambasted the methodology, objectivity, and transparency of the SBU study. Like Lucas et al., Narang and Greeley declared the triad a “strawman,” with the statement:
“Physicians experienced in the clinical evaluation of paediatric traumatic brain injury and AHT do not diagnose SBS by a ‘triad’.”
Narang and Greeley also found it “troubling” that the SBU panel “was offered and refused external peer review by no fewer than seven international professional medical societies” before the publication of their report, and charged that the panel was biased in two ways:
- One of the SBU panelists had testified before the highest court in Sweden, prior to the study, that “the diagnostic model of the ‘triad’ for diagnosing SBS ‘has been criticised’, and that ‘there is currently no clarity about the extent to which the components of the triad are specific to violent shaking’.”
- A former chair of the SBU had also testified in the same case, and “has openly expressed scepticism of the diagnosis of AHT because of his personal experiences with a family member being criminally charged in a suspected shaken baby case.”
Another “Different View” column published in May, by Dr. Robert A.C. Bilo and others, focused specifically on the papers used to support the study’s conclusion that the triad had many “alternative explanations.” Bilo et al. rejected the cases and papers cited in support of these explanations, with three main arguments:
- many of the cases would never have been diagnosed as abuse, because the children clearly suffered other medical conditions
- some of the cases did not fully conform to the triad
- some of the cases were in fact abuse misrepresented as organic causes
Like other critics, including Lucas et al., the Bilo authors accused the SBU of applying a double standard, because the reviewers accepted individual case reports as evidence for other causes, while they rejected studies with fewer than 10 cases from their main literature review.
Lynøe et al. clarified in their response that the papers cited as evidence for other causes had simply emerged during their literature review, and had been rejected from the main study for the same reasons as many others. They explained:
“From an epidemiological point of view, and due to random fluctuations, studies with less than 10 study cases are of very limited value. But when looking for differential diagnoses, one single case is sufficient to question the general assumption that when the triad is present the infant must have been violently shaken.”
The original study had addressed the question:
With what certainty can it be claimed that the triad, subdural hematoma, retinal hemorrhages and encephalopathy, is attributable to isolated traumatic shaking (i.e. when no external signs of trauma are present)?
The Acta Paediatrica treatment articulated the answer in two, subtly different conclusions. First:
“[T]here is insufficient scientific evidence on which to assess the diagnostic accuracy of the triad in identifying traumatic shaking (very low-quality evidence).”
That is, the literature supporting the opinion that the presence of the triad proves a child was shaken is “insufficient,” because none of the papers supporting that opinion ranked above “very low-quality.” Second:
“[T]here is limited scientific evidence that the triad and therefore its components can be associated with traumatic shaking (low-quality evidence).”
 That is, the researchers found some low-quality papers supporting the opinion that traumatic shaking causes the triad—two French papers based on confessions—but no medium- or high-quality papers. Before reaching their conclusions, the authors had read and evaluated 1,000 academic papers, only 30 of which met their inclusion criteria. They ranked 28 of those 30 papers as having a “high risk of bias,” 2 of them as having a “moderate risk,” and none of them as having a “low risk” of bias (a flow chart illustrating the literature search).
That is, the researchers found some low-quality papers supporting the opinion that traumatic shaking causes the triad—two French papers based on confessions—but no medium- or high-quality papers. Before reaching their conclusions, the authors had read and evaluated 1,000 academic papers, only 30 of which met their inclusion criteria. They ranked 28 of those 30 papers as having a “high risk of bias,” 2 of them as having a “moderate risk,” and none of them as having a “low risk” of bias (a flow chart illustrating the literature search).
In an over-reaching answer to their many critics, the Lynøe team called for a more scientific approach to research in the arena:
“We acknowledge the concerns expressed by all of the authors who responded with regard to child welfare and the possibility that the diagnoses may be delayed in individual cases of child abuse. However, we are very troubled by the disregard displayed by those authors to the significant methodological problems inherent in published research on shaken baby syndrome. With the exception of Ludvigsson, none of these authors expressed concern about the problems of circular reasoning, lack of comparison groups or the other methodological problems we identified in the systematic review. Where has all the critical thinking in research gone?…
“The purpose of a systematic review is to examine the quality of published research. With that in mind, please accept the substantial difficulties and limitations of previous research carried out by the ‘shaken baby syndrome’ and ‘abusive head trauma’ and help to add true knowledge by performing better research that overcomes the methodological problems.”
copyright 2017, Sue Luttner
If you are not familiar with the debate surrounding shaken baby syndrome/abusive head trauma, please see the home page of this blog.

 Pediatric neuropathologist Dr. Waney Squier has hit one out of the park in her TEDx talk, “I believed in Shaken Baby Syndrome until science showed I was wrong,” published Friday on Progress Video TV.
Pediatric neuropathologist Dr. Waney Squier has hit one out of the park in her TEDx talk, “I believed in Shaken Baby Syndrome until science showed I was wrong,” published Friday on Progress Video TV. The talk opens with the story of Linda, a mother convicted of shaking her third child to death based on the presence of the triad: bleeding in the retinas, bleeding beneath the lining of the brain, and brain swelling. “At her trial, Linda was described as a woman of good character, a caring and careful mother,” Dr. Squier recounts, “But doctors—medical experts—said that those three findings meant that [the boy] must have been violently shaken” when alone with his mother.
The talk opens with the story of Linda, a mother convicted of shaking her third child to death based on the presence of the triad: bleeding in the retinas, bleeding beneath the lining of the brain, and brain swelling. “At her trial, Linda was described as a woman of good character, a caring and careful mother,” Dr. Squier recounts, “But doctors—medical experts—said that those three findings meant that [the boy] must have been violently shaken” when alone with his mother. When Linda was first accused, the police had called in Dr. Squier, an expert on infant brain pathology. After examining the brain, she had endorsed the opinion of the other doctors, that it was a case of shaken baby syndrome. “They believed in it, and I believed in it,” she grimaces, “and so my report was part of the evidence that cost Linda so much.”
When Linda was first accused, the police had called in Dr. Squier, an expert on infant brain pathology. After examining the brain, she had endorsed the opinion of the other doctors, that it was a case of shaken baby syndrome. “They believed in it, and I believed in it,” she grimaces, “and so my report was part of the evidence that cost Linda so much.”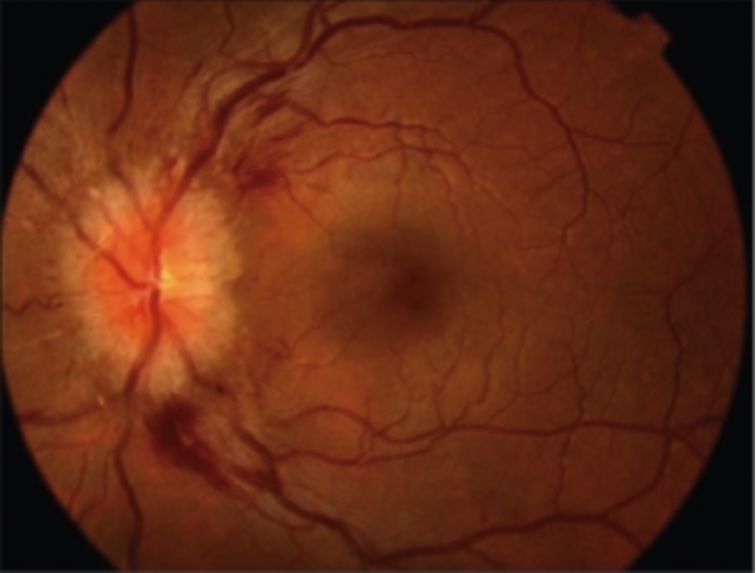

 The SBU team looked only at cases of pure shaking, without evidence of impact, in children younger than 12 months, and they set
The SBU team looked only at cases of pure shaking, without evidence of impact, in children younger than 12 months, and they set 