And in Florida, the First Coast News has been following the story of a controversial child abuse pediatrician who has now resigned, after leaving jobs in both Wisconsin and Alaska amid complaints like those raised in Florda:
These stories remind me of the parent activists in Leheigh Valley, Pennsylvania, who started organizing in 2023 against their local child abuse expert, ultimately forcing her resignation. My own posting about a report from their county assessor on the costs of misdiagnosis covers some of the group’s first public actions. The headlines from ABC Action News tell the larger tale:
Investigative journalist Pamela Colloff, in a first-rate article last winter in the New York Times (“He Dialed 911 to Save His Baby. Then His Children Were Taken Away“) weaves one family’s compelling story into an examination of the tensions between the physicians who diagnose abuse and the physicians who question the reliability of a Shaken Baby Syndrome diagnosis (now known as Abusive Head Trauma).
A couple of decades ago, after years tracking the footnotes through the medical literature, I concluded that shaken baby theory hit the courtroom before its scientific underpinnings were established, and then the pressures of litigation encouraged child-abuse experts to adopt and defend an early, flawed model of a complex physiological condition. The resulting convictions have calcified unproven core beliefs about both mechanism and timing. Parents of children with rare and misunderstood illnesses and injuries are still paying the price.
-Sue Luttner
If you are not familiar with the debate surrounding Shaken Baby Syndrome, please see the home page of this blog.
Following a flood of media coverage and days of intense legal maneuvering, Texas father Robert Roberson is still alive, after the state supreme court issued a temporary reprieve minutes before he was scheduled to be executed last evening.
All of Robert’s appeals and petitions had been denied, but on Wednesday the Criminal Jurisprudence Committee in the state’s House issued a subpoena for Roberson to appear for a hearing next Monday, a move that raised a jurisdictional dispute and led to a series of motions, counter-motions, and, eventually, a stay, for now.
“The vast team fighting for Robert Roberson – people all across Texas, the country, and the world – are elated tonight that a contingent of brave, bipartisan Texas lawmakers chose to dig deep into the facts of Robert’s case that no court had yet considered and recognized that his life was worth fighting for,” Roberson’s attorney Gretchen Sween said Thursday night.
Roberson enjoys the support of the Innocence Project; a number of physicians, scientists, and attorneys who question the SBS hypothesis; a majority of the Texas state legislators; and his own friends and family as well as other wrongly accused families, autism and disability-rights groups, and attorney/novelist John Grisham.
Meanwhile, the case has triggered local, national, and international media coverage, shining a much-needed spotlight on the debate surrounding Shaken Baby Syndrome. Some of the news treatments:
The scheduled execution of convicted father Robert Roberson in Texas on October 17 has inspired a surge of activism from around the world by doctors, lawyers, scientists, journalists, non-profits, and families wrongly accused of child abuse.
This month in D Magazine, in a story titled “Will Texas Kill This Innocent Man?”, best-selling novelist John Grisham lays out the medical complexities of the case, concluding that Roberson’s daughter died of natural and accidental causes, not Shaken Baby Syndrome (SBS).
The Innocence Project has launched a last-chance public petition, and a coalition of wrongly accused parents in Europe, Adikia, has stepped up not only to gather signatures from families internationally but also to promote an on-line symposium on SBS early next month, organized by the Cato Institute in response to the scheduled execution.
In July, The New York Times posted a video opinion piece by Rev. Brian Wharton, once the detective in charge of the investigation and now an advocate for Roberson’s innocence.
Wharton didn’t know at the time, he says, that Roberson is on the autism spectrum, which explains the “flat aspect” that had seemed consistent with the abuse diagnosis. “No other possibilities for her injuries were considered,” he sighs. “I deeply regret that we followed the easiest path.”
Earlier this week, Roberson’s defense team filed a clemency petition with Texas Governor Greg Abbott and the Texas Pardons Board, pulling together the medical, scientific, and legal arguments against the execution and providing a collection of support documents from medical and legal professionals, political and civil liberty organizations, autism and parent-support groups, 84 members of the Texas House of Representatives, and the mother of a former classmate of Roberson’s who describes him as “a gentle soul.”
Robert Roberson, an Autistic Father Wrongfully Convicted and Sentenced to Death in Texas Based on the Debunked “Shaken Baby Syndrome” Hypothesis, Applies for Clemency to Stop his October 17th Scheduled Execution
Medical and Scientific Experts, Bipartisan Texas Lawmakers, Advocates for Parental Rights, Autism Organizations, Best-Selling Novelist John Grisham, Former Lead Detective Brian Wharton, Innocence Groups, the Texas Catholic Conference of Bishops, and Dozens of Others Urge Texas Pardons Board to Recommend, and Gov. Greg Abbott to Grant, Clemency
(Austin, Texas, Tuesday, September 17, 2024) Today, 34 eminent scientists and doctors, a bipartisan group of 84 Texas legislators, 8 advocates for parental rights, 8 organizations that advocate for people with Autism and their families, faith leaders, innocence advocacy groups, former judges, 70 attorneys who have represented people wrongfully accused of child abuse, and former lead detective Brian Wharton, among others, filed letters in support of Robert Roberson’s clemency petition to the Texas Board of Pardons and Paroles and Governor Greg Abbott. (Exhibits 7, 15-23.)
Mr. Roberson’s petition describes the new medical and scientific evidence that his jury never heard showing that no homicide occurred. Mr. Roberson’s two-year-old, chronically ill daughter, Nikki, actually died of severe viral and bacterial pneumonia that medical professionals missed in 2002, not because of any abuse. Her illness progressed to sepsis and then septic shock, a process likely precipitated by the dangerous respiratory-suppressing medications she was prescribed during her last days, all of which has now been established by detailed reports from highly qualified medical specialists.
No court has been willing to consider three new expert reports showing how Nikki died of pneumonia, proof that Mr. Roberson is innocent of any crime.
The power of Mr. Roberson’s innocence claim is attracting diverse and widespread support, including from best-selling novelist John Grisham, who said, “This isn’t a case where the system got the wrong guy, but rather one where no crime took place at all. Something must be done to stop Robert’s execution. Governor Abbott and the Board of Pardons and Paroles can prevent an irreparable injustice by granting him clemency.”
Brian Wharton, the lead detective in charge of investigating Nikki’s death who directed that Mr. Roberson be arrested based on a doctor’s Shaken Baby hypothesis made even before an autopsy was performed, and who testified for the prosecution at trial, has come to believe Mr. Roberson is innocent and has filed a letter of support, urging clemency.
“I will forever be haunted by the role I played in helping the State put this innocent man on death row,” said Brian Wharton. “Robert’s case will forever be a burden on my heart and soul. But it is not too late for Texas to change course and stop his execution. I sincerely hope that Governor Abbott and the Board will step in to do so.” (See also Exhibit 7.)
Mr. Roberson is scheduled for execution on October 17, 2024, and is at risk of being the first person in the United States executed based on the discredited “Shaken Baby Syndrome” hypothesis, unless the courts or Governor Abbott intervenes.
A combination of Nikki’s undiagnosed pneumonia, medications that suppressed her breathing, an accidental fall, and the medical triage undertaken after her collapse entirely explain Nikki’s condition.
Mr. Roberson’s clemency petition states:
“Nikki’s death … was not a crime—unless it is a crime for a parent to be unable to explain complex medical problems that even trained medical professionals failed to understand at the time. We now know that Nikki’s lungs were severely infected and straining for oxygen—for days or even weeks before her collapse. A recent reexamination of lung tissue collected during her autopsy has revealed that both a chronic interstitial viral pneumonia and a secondary acute bacterial pneumonia were ravishing her lungs, causing sepsis and then septic shock.
“In the days before her collapse, Robert repeatedly took Nikki to the local Emergency Room (ER) and to her pediatrician in rural Palestine, Texas, seeking help. But unaware of her severe pneumonia, doctors sent her home with medications that would only have made her condition worse. As an expert in medical toxicology has now explained, the medications prescribed to her—Phenergan (the brand name for promethazine) and codeine—would only have further suppressed Nikki’s ability to take in oxygen. Codeine is a narcotic, not recommended for anyone under age eighteen; Phenergan now has FDA “black box warnings” against prescribing it to children Nikki’s age and in her condition precisely because it can suppress breathing and result in death. These potent, respiratory-suppressing drugs certainly were not designed to treat a toddler’s severe respiratory illness, i.e., pneumonia.” (Petition at pp. 4-5.)
On the night of January 30, 2002, Mr. Roberson heard a “strange cry” and woke up to find Nikki lying on the floor at the foot of the bed. Mr. Roberson comforted Nikki and wiped a small speck of blood off her mouth but did not observe anything else wrong. They eventually fell back asleep. But when he woke up a few hours later, Mr. Roberson found Nikki unconscious with blue lips. He was horrified and tried to revive her. Then he took her to the ER.
More than 30 medical and scientific experts have written to the Board of Pardons and Paroles stating:
“There was no differential diagnosis undertaken at that time because, in 2003, presuming abuse was recommended pursuant to the Shaken Baby Syndrome hypothesis, then treated as medical orthodoxy. Today, no reputable medical doctor would fail to conduct a thorough, multi-disciplined exploration of all possible causes of death because it is now known that many phenomena—including accidental short falls and naturally occurring disease—can cause the same intracranial conditions that ‘mimic’ inflicted head injury.” (Petition at Exhibit 15.) If Nikki died today, instead of presuming Nikki’s condition was caused by abuse, no doctor would consider Shaken Baby Syndrome as the cause of Nikki’s death because SBS is now considered a diagnosis of exclusion; Nikki’s pneumonia, the extreme levels of dangerous medications found in her system during her autopsy, and her fall from the bed explain why Nikki died.
Mr. Roberson’s Autism – which was not known to the hospital staff and was not diagnosed until 2018 – played a pivotal role in the rush to judgment in his case.
Hospital staff interpreted Mr. Roberson’s seemingly blank reaction to Nikki’s serious condition as callousness, when in fact his Autism explained his non-neurotypical response to the emergency. (Petition at Exhibit 17) (Letter of support from eight state and national advocacy groups for people with Autism and their families.)
“Robert Roberson’s Autism, which affects social and emotional processing, led to a lack of visible emotional response—a characteristic misinterpreted during his trial as a sign of guilt,” said Christopher Banks, President and CEO of the Autism Society of America. “This tragic misjudgment, combined with the absence of expert testimony on Autism, culminated in a wrongful conviction, in which we urge Governor Abbott to grant clemency.”
“The prosecution’s reliance on misjudgment and bias against Mr. Roberson’s Autistic behavior suggests a rush to judgment substantially influenced by criminalizing disability,” said Jacquie Benestante, Executive Director of the Autism Society of Texas. “We are calling for justice and clemency, urging Governor Abbott and the Board of Pardons and Paroles to consider the compelling evidence and prevent a wrongful execution.”
A bipartisan group of 84 Texas lawmakers wrote the Board separately this week, urging it to recommend clemency for Mr. Roberson “out of grave concern that Texas may put him to death for a crime that did not occur.”
The lawmakers emphasized that, more than 10 years ago, the Texas House unanimously passed a law to allow challenges to convictions based on disproven or incomplete science. They have been “dismayed to learn that this law has not been applied as intended and has not been a pathway to relief – or even a new trial – for people like Mr. Roberson. In his case, significant scientific and medical evidence now shows that his daughter Nikki, who was chronically ill, died of a combination of natural and accidental causes, not the debunked shaken baby syndrome hypothesis the State used to convict Mr. Roberson.” (Exhibit 16.)
The lawmakers further emphasized that the House also passed a law in 2021 “which now ensures that parents have the right to a second expert medical opinion after allegations of child abuse. Had these events occurred today, Mr. Roberson would have been legally entitled to an additional medical review at his request.” (Exhibit 16.)
Eight advocates for parental rights wrote to the Governor and the Board that Mr. Roberson’s case “demonstrates a shocking disregard for his parental rights.” They explained:
“Abuse was the default – and wrong – assumption before any determination was made about Nikki’s medical condition. Mr. Roberson was viewed with suspicion from the outset because of symptoms associated with his then-undiagnosed autism spectrum disorder.
“Because of these egregious factors, Mr. Roberson was denied the ability to see Nikki in the hospital, and he was arrested before an autopsy was even performed. What’s more, Mr. Roberson was not advised of any end-of-life decisions being made for Nikki despite having full custody … Clemency is necessary to prevent the irreparable harm of executing this innocent parent.” (Exhibit 18.)
Mr. Roberson’s clemency petition includes numerous letters of support from his spiritual advisors, friends, and supporters who attest to his faithful, peaceful and loving nature.
He has completed some 60 different Bible study courses and has had a virtually pristine disciplinary record during his many years in prison. Because of his record of peacefulness, he was selected to be in the very first faith-based program on death row. In addition, he was one of only 13 men selected to participate in an experimental “group rec” program that allowed him to move freely on the pod with others determined to be no threat to anyone. (Petition at p. 38, 52.) Many people attest to his empathy and concern for others over himself. For example, his spiritual advisor, Donna Drake Farmer, has written that Mr. Roberson’s support for her while she was caring for her dying husband gave her peace and that Mr. Roberson “probably knows more of my concerns and worries than my birth children do.” (Petition at p. 56, Exhibit 23.)
An overview of Robert Roberson’s innocence case is here.
A photo of Mr. Roberson can be accessed here. Source: Roberson Family.
Watch New York Times Opinion Video showing meeting between lead detective Brian Wharton and Robert Roberson here.
Arizona trial attorney Randy Papetti has brought nearly 20 years of experience and research to his valuable new analysis of shaken baby theory in the courtroom, The Forensic Unreliability of the Shaken Baby Syndrome, now shipping from Academic Forensic Pathology International.
Papetti is not a criminal attorney but a recognized leader in his primary field, commercial litigation. In 2013, he was selected by Best Lawyers and his local peers as the Lawyer of the Year for “Bet-the-Company Litigation.” In 2011, he was inducted into the invitation-only American College of Trial Lawyers. His shaken baby work has all been pro bono.
Randy Papetti
Papetti was only doing a favor for a friend, he told me in a telephone interview, when he agreed to help with his first alleged shaking case, an appeal of a murder conviction. The convicted father had reported a fall from a high chair, but the child abuse experts had insisted that shaking must have been involved. Papetti started researching the medical and legal arguments, he said, and found himself face to face with the difference between medical opinion and proven scientific fact.
Drayton Witt and his wife, courtesy Arizona Justice Project
Papetti won that appeal, and other attorneys started approaching him with their own shaking cases. He was a key player in the 2012 freeing of Drayton Witt, whose son died after a short lifetime of serious health problems, including a seizure disorder. It was the Witt case that brought pioneering pediatric neurosurgeon Dr. Norman Guthkelch back into the arena, four decades after he lay the groundwork for the diagnosis by proposing that shaking an infant could cause subdural bleeding. Like Papetti, Dr. Guthkelch rejected the medical thinking that had convicted Drayton Witt. Guthkelch then spent the final years of his life fighting what he considered a “tragic misinterpretation” of his work.
“Witt was a powerful case,” Papetti said. “It showed how easily a mistaken diagnosis based on the ‘triad‘ can convict.” By then law professor Deborah Tuerkheimer had published her first journal argument against shaking theory, and her New York Times op ed. Papetti thought the tide was turning. “The information was out there, people could see that shaking theory was unreliable.”
Instead of reconsidering their model, however, proponents of shaking theory “took a course I never imagined they would be able to take, claiming there never was a triad,” Papetti marveled in our interview. In his book, he noted that changing the name of the diagnosis from “shaken baby syndrome” to “abusive head trauma” did not address the fundamental problem that the entire theory was speculation. “It merely changed the diagnosis’ name for legal purposes.”
Papetti said he was “stunned” to see how child abuse professionals have lashed out personally at defense experts and attorneys: ridicule at conferences, perjury charges, letters to employers. “That’s not the way the game is played,” he said. Attorneys in civil practice fight hard in the courtroom, he claimed, but can still respect their opponents professionally and maintain personal friendships.
In his book, Papetti traces the evolution of shaking theory in both the medical literature and the courts. He illustrates how the two have co-evolved, distorting each other, and he examines the cooperative relationship among child abuse experts, the police, and social services. He writes:
These institutional realities, not science or clinical validation, best explain how SBS has persisted and why the medical profession is unlikely to correct it any time soon.
“Things tend to get worse before they get better,” he told me, “And I’m afraid that’s where we are now, still getting worse.” At this point, proponents of shaking theory staff the medical schools and the childrens’ hospitals, dominate the professional organizations, and conduct the bulk of the research. Critics tend to be independent thinkers who have researched the literature and reached their own conclusions. “The imbalance of power has distorted everything completely,” Papetti said. “At the end of the day, are you really asking a judge to not allow the testimony of these luminaries because a few brave souls disagree?”
So he keeps chipping away at a calcified theory with the facts, hoping to explain it all clearly enough that judges will see how decades of unproven medical testimony have led to a criminal justice crisis of staggering proportions.
Pediatric neuropathologist Dr. Waney Squier has hit one out of the park in her TEDx talk, “I believed in Shaken Baby Syndrome until science showed I was wrong,” published Friday on Progress Video TV.
While telling her own story with calm, compelling intensity, she also describes the pain inflicted on innocent families by misguided accusations of abuse and documents the refusal of the legal and medical communities to accept the unwelcome truth about their flawed theory.
“By ignoring the science and adopting an unproven hypothesis, doctors have done great harm,” she concludes, “and have led the courts astray.”
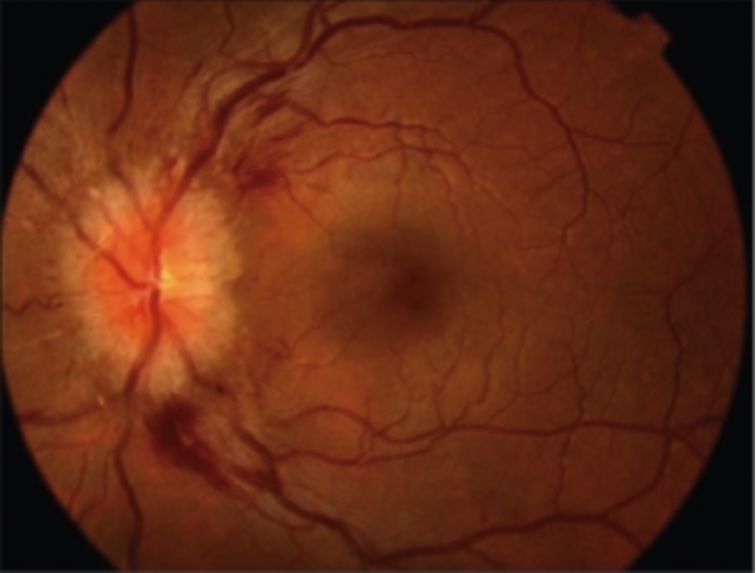
The talk opens with the story of Linda, a mother convicted of shaking her third child to death based on the presence of the triad: bleeding in the retinas, bleeding beneath the lining of the brain, and brain swelling. “At her trial, Linda was described as a woman of good character, a caring and careful mother,” Dr. Squier recounts, “But doctors—medical experts—said that those three findings meant that [the boy] must have been violently shaken” when alone with his mother.
Three years later, Linda’s conviction was overturned on appeal. “Her name was cleared, but her life was ruined,” Squier says. Her parents had died and her husband had left her. Her fourth child, a little girl born in prison, had been taken from her at birth and placed for adoption, and even after her exoneration, Linda was prohibited from attempting contact.
When Linda was first accused, the police had called in Dr. Squier, an expert on infant brain pathology. After examining the brain, she had endorsed the opinion of the other doctors, that it was a case of shaken baby syndrome. “They believed in it, and I believed in it,” she grimaces, “and so my report was part of the evidence that cost Linda so much.”
Dr. Squier says her own doubts about shaking theory started when another neuropathologist, Dr. Jennian Geddes, published research suggesting that the damage in presumed shaking cases resulted from lack of oxygen, not from direct violence. Dr. Squier recalls:
“Back in 2001, the Geddes research stopped me in my tracks. It wasn’t what I had expected. So I read everything I could about shaken baby syndrome, and as a scientist, I’m embarrassed to admit to you I hadn’t done so before. I’d been making this diagnosis on the basis of my uncritical acceptance of what was in the textbooks and what I’d been taught. I was startled to learn that there was no scientific foundation for the hypothesis.”
No one has ever witnessed a shaking assault that resulted in the triad, she reports. Laboratory research and biomechanical calculations have only cast doubt on the theory, and past experience with front-facing car seats tells us that whiplash forces cause fractures and dislocations in the neck, not intracranial bleeding and swelling.
After her realization that the theory was not only unproven but likely wrong, Dr. Squier started conducting her own research, and she started testifying for the defense. But her willingness to speak out against the common knowledge resulted in criticism from colleagues,scoldings from judges, and complaints to the authorities. In the spring of 2016, after hearings triggered by a police complaint to the General Medical Council, she temporarily lost the right to practice medicine, until a higher court reinstated her, declaring most of the first findings “unsustainable.” She is still prohibited from testifying in British courts for another year and a half.
The actions against her have successfully stifled the voices of dissent, Dr. Squier argues, leaving innocent families “defenseless” against their accusers. “Back in 2005, Linda had seven medical experts to support her. Today she would be likely to have none.”
Some other key points from Dr. Squier’s talk:
“So today, as I stand here, I am sure that shaking can harm babies, and we certainly shouldn’t shake babies. But nearly 50 years of research has failed to provide us with the justification to make the assumption that a baby who has the triad or any of its components must have been shaken.”
“If we do nothing, then ordinary people, people who have already suffered the tragedy of the death of a baby, will continue to have their families torn apart by incorrect and unscientific opinions…
“If we do nothing, this travesty will continue… this willful refusal of the courts and the doctors advising them to recognize the science that shows they are wrong.”
But you might have other favorite quotes. I suggest you watch the entire talk.
Copyright 2018, Sue Luttner
If you are not familiar with the debate about shaken baby theory, please see the home page of this blog.
The July issue of Acta Paediatrica offers a collection of free, live links to a volley of rebuttals published over the past four months to an article in March submitted by medical ethicist Dr. Niels Lynøe and most of the other experts who informed the 2016 Swedish report critical of shaking theory, commissioned by an independent agency in Sweden whose name is abbreviated SBU.
In an email exchange last week, Dr. Lynøe wrote that his team knew the topic was controversial, but they were “rather surprised” at the vehemence of the criticisms. “I also think that there was something positive with the critical comments,” he added, “because we got the opportunity to explain and explore some aspects more.”
Dr. Niels Lynøe
The March paper reported on the same research as the SBU study, an exhaustive evaluation of the shaken baby literature that ultimately declared the scientific evidence behind shaking theory “weak.” The analysis noted fundamental problems with the bulk of the published research—in a typical study design, the report noted, researchers had applied the criteria they were attempting to prove when identifying and sorting their subjects, so the results necessarily supported their theory.
Weeks after the Lynøe et al. paper appeared, Acta Paediatrica published an editorial by epidemiology professor Jonas F. Ludvigsson criticizing the SBU’s methods and warning of an “imminent risk” that the paper will discourage the reporting of child abuse and leave abused children undiagnosed. Dr. Ludvigsson conceded quality problems with past SBS research, but rejected the SBU’s conclusions and endorsed reliance on the triad:
“[The study’s] publication in Acta Paediatrica does not spell the end of the discussion. Instead, it is a clear signal that more research is needed. But for now, paediatricians should continue to alert social services when they observe a child with the triad, once other explanations for subdural haematomas, retinal haemorrhages and brain ischaemia and oedema have been ruled out.”
The next critique of Lynøe et al., in mid April, added irony to the collection by denying the triad itself. An editorial by violence and abuse specialist Dr. Steven Lucas and others charged that the SBU’s methods had become “untethered from the agency’s published methodology” and argued that the study was fundamentally flawed, because it had examined the question of whether the presence of the triad proves infant shaking. Lucas et al. wrote:
“The construct of the ‘triad’ represents a rhetorical fallacy known as a straw man, which gives the impression of refuting an opponent’s argument – the ‘triad’ is pathognomonic for AHT – when, in fact, that argument was never advanced by that opponent. We maintain that the term ‘triad’ carries no value for clinicians experienced in evaluating suspected AHT.”
In refutation of the straw man argument, I point out that both Joshua Burns and Michelle Heale were convicted based only on the opinion of child abuse experts that the triad proves abusive head trauma—these cases are not unique, only easy to reference here. I myself have researched dozens of convictions based on the triad, sometimes on only one or two elements of the triad.
Lynøe et al. addressed the straw man argument in a response to a different criticism (the response to Narang et al.), by quoting these physician guidelines, which clearly endorse the triad:
“If there is no history of traffic accident or fall from a considerable height, the combination of subdural hematoma and encephalopathy with edema or hemorrhage strongly suggest that the infant has been abused. If there are also retinal hemorrhages then from the medical point of view the diagnosis of abuse is quite clear.”
Also in April, Acta Paediatrica published an editorial by pediatric ophthalmologist Dr. Alex Levin, who declared, “There is a plethora of scientific evidence that retinal hemorrhages are a cardinal feature of abusive head trauma.” Among other objections to the study, he criticized the SBU’s failure to consider the various possible sizes and locations of retinal hemorrhages. “To ignore these descriptors,” he wrote, “is like saying that a rose is no different than any other ‘flower.'”
Dr. Levin also objected that the SBU team had ignored the “wealth of clinical experience” available from the community of child abuse experts. He argued that certain retinal findings, even in the absence of any other evidence, should shift the assumption to one of abuse:
“A diagnosis of abuse should not be made solely based on retinal haemorrhages, but certain retinal findings make that likelihood dramatically high, so high that one must actively seek (or rule out) supportive evidence that the child has been abused and is in need of protection.”
Another commentary in the April issue, by eye and vision specialist Dr. Kerstin Hellgren and others, called the SBU report “misleading.” In an apparent endorsement of both the triad and the literature that supports it, the authors wrote:
“The SBU report concludes that there is only limited evidence that shaking of an infant can cause the triad signs, in contrast with the numerous reports describing such lesions in victims of verified shaking. It is unfortunate that the SBU panel neither included a paediatrician nor a paediatric ophthalmologist with experience of child abuse to facilitate a correct interpretation of the cited papers.”
In a response to both Levin and Hellgren et al., the Lynøe authors reiterated their commitment to objectivity:
“If physicians involved in child protection teams embraced the research question as if it was a generally accepted scientific fact when classifying cases and controls, this would have resulted in circular reasoning when estimating the diagnostic accuracy of the triad. For that reason, and in order to avoid conflicts of interest and circular reasoning, the expert panel did not include any experts associated with child protection teams. The panel comprised two paediatricians and one expert each from the fields of forensic medicine, radiology, epidemiology and medical ethics. All the included had long experience of assessing scientific work and were scrutinised for potential conflicts of interest and cleared by the Agency. The expert panel followed the guidance in handbooks for assessing health technology and any other panel reproducing the study would have probably arrived at the same conclusions.”
In May, Dr. Sandeep Narang and Dr. Christopher Greeley, both renowned child abuse specialists, published a column in the Acta Paeditrica series “A Different View” that lambasted the methodology, objectivity, and transparency of the SBU study. Like Lucas et al., Narang and Greeley declared the triad a “strawman,” with the statement:
“Physicians experienced in the clinical evaluation of paediatric traumatic brain injury and AHT do not diagnose SBS by a ‘triad’.”
Narang and Greeley also found it “troubling” that the SBU panel “was offered and refused external peer review by no fewer than seven international professional medical societies” before the publication of their report, and charged that the panel was biased in two ways:
One of the SBU panelists had testified before the highest court in Sweden, prior to the study, that “the diagnostic model of the ‘triad’ for diagnosing SBS ‘has been criticised’, and that ‘there is currently no clarity about the extent to which the components of the triad are specific to violent shaking’.”
A former chair of the SBU had also testified in the same case, and “has openly expressed scepticism of the diagnosis of AHT because of his personal experiences with a family member being criminally charged in a suspected shaken baby case.”
Another “Different View” column published in May, by Dr. Robert A.C. Bilo and others, focused specifically on the papers used to support the study’s conclusion that the triad had many “alternative explanations.” Bilo et al. rejected the cases and papers cited in support of these explanations, with three main arguments:
many of the cases would never have been diagnosed as abuse, because the children clearly suffered other medical conditions
some of the cases did not fully conform to the triad
some of the cases were in fact abuse misrepresented as organic causes
Like other critics, including Lucas et al., the Bilo authors accused the SBU of applying a double standard, because the reviewers accepted individual case reports as evidence for other causes, while they rejected studies with fewer than 10 cases from their main literature review.
Lynøe et al. clarified in their response that the papers cited as evidence for other causes had simply emerged during their literature review, and had been rejected from the main study for the same reasons as many others. They explained:
“From an epidemiological point of view, and due to random fluctuations, studies with less than 10 study cases are of very limited value. But when looking for differential diagnoses, one single case is sufficient to question the general assumption that when the triad is present the infant must have been violently shaken.”
The original study had addressed the question:
With what certainty can it be claimed that the triad, subdural hematoma, retinal hemorrhages and encephalopathy, is attributable to isolated traumatic shaking (i.e. when no external signs of trauma are present)?
The Acta Paediatrica treatment articulated the answer in two, subtly different conclusions. First:
“[T]here is insufficient scientific evidence on which to assess the diagnostic accuracy of the triad in identifying traumatic shaking (very low-quality evidence).”
That is, the literature supporting the opinion that the presence of the triad proves a child was shaken is “insufficient,” because none of the papers supporting that opinion ranked above “very low-quality.” Second:
“[T]here is limited scientific evidence that the triad and therefore its components can be associated with traumatic shaking (low-quality evidence).”
That is, the researchers found some low-quality papers supporting the opinion that traumatic shaking causes the triad—two French papers based on confessions—but no medium- or high-quality papers. Before reaching their conclusions, the authors had read and evaluated 1,000 academic papers, only 30 of which met their inclusion criteria. They ranked 28 of those 30 papers as having a “high risk of bias,” 2 of them as having a “moderate risk,” and none of them as having a “low risk” of bias (a flow chart illustrating the literature search).
In an over-reaching answer to their many critics, the Lynøe team called for a more scientific approach to research in the arena:
“We acknowledge the concerns expressed by all of the authors who responded with regard to child welfare and the possibility that the diagnoses may be delayed in individual cases of child abuse. However, we are very troubled by the disregard displayed by those authors to the significant methodological problems inherent in published research on shaken baby syndrome. With the exception of Ludvigsson, none of these authors expressed concern about the problems of circular reasoning, lack of comparison groups or the other methodological problems we identified in the systematic review. Where has all the critical thinking in research gone?…
“The purpose of a systematic review is to examine the quality of published research. With that in mind, please accept the substantial difficulties and limitations of previous research carried out by the ‘shaken baby syndrome’ and ‘abusive head trauma’ and help to add true knowledge by performing better research that overcomes the methodological problems.”
copyright 2017, Sue Luttner
If you are not familiar with the debate surrounding shaken baby syndrome/abusive head trauma, please see the home page of this blog.
Physicians and attorneys in Boston, Massachusetts, where the Louise Woodward trial brought shaken baby theory onto the national stage, are heading into another battle over infant shaking, as pediatricians clash with the medical examiner about the diagnosis and the state’s high court reconsiders past convictions.
Aisling Brady McCarthy
Tensions started ramping up last summer, when the medical examiner’s office changed the cause of death in the case of 1-year-old Rehma Sabir, from “homicide” to “undetermined,” which convinced the district attorney to drop murder charges against the girl’s nanny, Irish national Aisling Brady McCarthy. Not quite a year earlier, with less publicity but for the same reason, the county had dropped charges against accused father Geoffrey Wilson. Then last December, the medical examiner’s office pulled back from a third homicide declaration in an infant death initially attributed to shaking, but the district attorney held firm and is still moving forward with charges against Pallavi Macharla, a child care provider who had been a physician in her native India.
Now the Massachusetts chapter of the American Academy of Pediatrics (AAP) has written a letter to Governor Charlie Baker calling for an investigation of the medical examiner’s office and warning that its staff might be listening to the opinions of defense experts, as quoted by Patricia Wen in The Boston Globe:
“Publicly available information questions whether individual examiners may have been influenced by participating attorneys and paid reports from defense medical experts,” according to the letter obtained by the Globe. “Sadly these extraordinary and alarming events call into question both the capacity and independence of our medical examiner’s office.”
This quote illustrates the kind of rhetorical thinking that can obscure logic when the topic is child abuse. Despite the implications of the phrase “paid reports from defense medical experts,” the state’s doctors are also paid for the time they spend preparing reports. The objection, then, must rest on who is paying, as if the opinions of the state’s doctors should necessarily prevail over the opinions of the defense experts. And I wonder whether the pediatricians have really thought through the question of “independence.” The medical examiner’s office is ordinarily on the same team as the detectives and the prosecutors, all agents of the state. In child abuse cases, the diagnosing pediatricians are also part of the prosecution team. In three instances in less than two years now, individual examiners have concluded that medical factors identified by defense doctors could have explained the infant deaths, putting the examiners at odds with physicians who are usually their allies. To me, that sounds like the essence of independent thinking.
The Massachusetts pediatricians seem to be asking the governor to step in and order the medical examiner’s office to follow the advice of the child abuse experts. Again from The Boston Globe coverage:
“The letter to the governor appears to represent growing frustration by the pediatricians’ organization, which had originally sought a behind-the-scenes solution to their concerns that fatalities from abusive head trauma — also known as ‘shaken baby syndrome’ — were potentially being wrongfully labeled as deaths caused by rare medical events….
“In early March, top members of the pediatricians’ group met privately with state public safety secretary Daniel Bennett and [Dr. Henry] Nields, the chief medical examiner, hoping they would agree to launch a comprehensive review of the handling of these child fatalities.
“Instead, Bennett later suggested to the pediatricians’ group that they ‘prepare a presentation’ for the pathologists at the medical examiner’s office. In response, in a letter dated April 29, the pediatricians’ group went directly to the governor demanding a review.”
In a follow-up debate on station WGBH in Boston, former Massachusetts attorney general Martha Coakley, who prosecuted British au pair Louise Woodward in 1997, insisted that the pediatricians were right in the first place, the medical examiner’s office “doesn’t have the training to make the right decision” in abuse cases, and individual medical examiners are “just not doing their jobs.” She dismissed critics of shaken baby theory as “15 to 20 people who have made a cottage industry out of attacking these diagnoses.”
The letter to the governor was signed by Dr. Michael McManus, president of the Massachusetts chapter of the AAP, and Dr. Stephen Boos, chairman of the chapter’s abuse and neglect panel and a proponent of shaken baby theory. In a break-out session at the 2012 conference of the National Center on Shaken Baby Syndrome, Dr. Boos criticized both the structure and the implementation of the 2011 Jumparoo study by biomechanic John Lloyd, PhD, which concluded that a child playing in a commercial jumping toy achieved the same magnitude of angular acceleration as adult volunteers shaking a biofidelic mannequin. “Shaking is no worse than a Jumparoo?” Boos jeered, “You’ve got to be kidding me.” In a review of Dr. Steven Gabaeff’s 2011 article challenging the pathophysiological connection between brain findings and a shaking diagnosis, Dr. Boos acknowledged Dr. Gabaeff’s scholarship but rejected his “teleological flights of fancy,” summarizing:
“I do not believe this paper develops a larger truth, though there are kernels of truth here and there. Instead, it displays the sorts of arguments we must refute when asserting the mainstream view of abusive head trauma.”
A month after the pediatricians’ complaint to the governor, the Massachusetts Supreme Judicial Court (SJC) recognized the reality of a debate about shaken baby theory, in its decision ordering a new trial for Oswelt Millien, a father who served five years in prison for the presumed 2009 shaking of his daughter. The court concluded that Millien’s attorney had provided ineffective assistance by failing to seek court funds to hire an expert witness for an indigent defendant, so that the opinions of the state’s experts went unchallenged at trial—that is, the same situation the pediatricians would like to see in the medical examiner’s office.
If the district attorney follows through with a trial of Pallavi Macharla, though, I expect both sides to bring experts to the courtroom. Macharla’s attorney JW Carney demonstrated in the debate with Martha Coakley that he’s already done his homework (probably when representing Geoffrey Wilson), but in case he hadn’t, he could look to the Millien opinion, which features in its footnotes a bibliography of key documents in the shaking debate. Millien’s previous appeal had been turned down by a judge who agreed he deserved a defense expert but concluded that a single expert would not have changed the outcome of the trial. In this decision, the judges conclude that the jury might have made a different decision if they had known the diagnosis is controversial:
By vacating the defendant’s convictions in this case and ordering a new trial, we do not claim to have resolved the ongoing medical controversy as to how often the triad of symptoms of abusive head trauma are caused by accidental short falls or other medical causes. We are simply recognizing that there is a vigorous debate on this subject, that arguments are being made on both sides with support in the scientific and medical literature, that this debate is evolving, and that, in the circumstances of this case, we do not have confidence in the justice of these convictions where defense counsel did not retain an expert to evaluate the medical evidence and, as a result, the jury heard only one side of this debate.
Because Oswelt Millien has already served his term, the state has little incentive to pursue a second trial, but the debate will be through the headlines again, both as the Macharla case unfolds and when the SJC reaches a decision on the pending appeal of Derick Epps, convicted in 2007 of assaulting his girl friend’s daughter.
Meanwhile, the pediatricians are asking for an investigation of the medical examiner’s office. Myself, I am hoping for an investigation of the child abuse professionals who don’t understand the difference between “the mainstream view of abusive head trauma” and established scientific fact.
A Washington state appeals court has granted a new trial to Heidi Fero, a mother and babysitter who was out of prison but still under court supervision on a child assault conviction when her appeal was heard. The decision, written for the 3-judge panel by Judge Linda CJ Lee, recognizes a change in medical thinking about both the timing of infant head injuries and the reliability of an abuse diagnosis in these cases. Specifically, the decision endorses this defense argument:
[N]ew material facts exist in the form of the now generally accepted medical paradigm that recognizes children can remain lucid for up to three days after suffering similar head injuries and those injuries are now known to be caused by much less extreme circumstances.
On a January evening in 2002, Fero was caring for pair of siblings, a 15-month-old girl and a 4-1/2-year-old boy, as well as her own two young children. At about 7:45 pm, she called the children’s father to report that the boy had been seen “pushing [his sister’s] head into the wall.” She says she comforted the little girl and, when she seemed to fall asleep, put her on a futon.
At 9:54 p.m., Fero called 911, after she noticed that the girl’s eyes were half-open and she could not be awakened. When the ambulance arrived at 9:59, the child was completely unconscious.
At the hospital, doctors found subdural hematoma, cerebral edema, and retinal hemorrhages. According to the case summary, six prosecution doctors testified at trial that the findings could result only from a major trauma like a car accident, a long fall, or abuse by an adult, and that the child would have become unconscious almost immediately after the assault. Several of the experts seem to have specified that the girl had been violently shaken.
Fero was initially sentenced to 15 years, 5 years above the statutory limit because of the “special circumstances” of the infant victim’s extreme vulnerability and Fero’s failure in her “duty to protect” a child in her care. A 2005 decision reduced her sentence to 10 years, with the objection that the judge had not submitted the special circumstances to the jury for adjudication before applying them.
The 2014 petition that reversed Fero’s conviction included affidavits from two physicians, pediatric neuroradiologist Patrick Barnes, who testified for the prosecution in the highly publicized 1997 trial of “Boston nanny” Louise Woodward, and forensic pathologist Janice Ophoven, who has testified that shaken baby syndrome is “controversial” and “an ongoing debate in the medical field.”
The Fero decision offers this quote from Dr. Barnes, “Over the past decade, many doctors—including myself—have changed their testimony and beliefs to bring them into accord with the scientific evidence and standards of evidence-based medicine.” And on the subject of timing:
Given the new medical research on lucid intervals, the testimony of the State’s experts to the effect that [the girl] would have immediately gone unconscious is unsupported by the medical literature. It is impossible to tell from the radiology or otherwise in the medical record when [the girl] was injured, and there is a significant chance that she was injured before she arrived at Ms. Fero’ s home.
In her statement, Dr. Ophoven cited the 2001 position papers by the American Academy of Pediatrics (AAP) and the National Association of Medical Examiners (NAME) to support her contention that the testimony at Fero’s trial in 2003 reflected the thinking of the medical community at the time. The AAP position paper has been superseded, however, by a 2009 statement that recommended clinicians avoid the term “shaken baby syndrome,” in favor of the more general “abusive head trauma,” and contained no specifics about diagnosing the condition or timing the injuries. The NAME paper expired without renewal and has not yet been replaced.
The decision quotes Ophoven’s summary:
[I]t is my opinion that much of the medical testimony presented during Ms. Fero’ s 2003 trial is no longer scientifically valid in light of recent advances in the medical community’ s understanding of the natural, accidental and non-accidental causes of cerebral edema, subdural hematoma and retinal hemorrhages.
Ophoven also concluded that the child had probably suffered her head injury about 12 hours before the first CT scan, that is, before she had been dropped off at Fero’s house.
In his statement opposing Fero’s petition, prosecuting attorney Anthony Golik did not address the question of whether medical opinion has indeed changed, focusing instead on the timing of the petition and the argument that new opinions by new experts should not constitute “newly discovered evidence” for the purposes of re-opening a case:
Every murder, serious assault, rape, etc, would be subject to vacation and retrial whenever a defendant found an expert to write an affidavit indicating there were new scientific theories which would explain the evidence in such a way as to possibly exonerate the defendant. This simply cannot be the standard this Court applies in Fero’s situation. A new medical opinion or a new medical theory is not a “material fact.”
Although the filing came more than a decade after her conviction, the judges concluded that Fero had exercised “reasonable diligence” regarding timeliness, considering that she was in prison when the medical debate was building and needed time after her release to find an attorney who could research the debate. The decision cited four other cases in the past few years where the convictions of child care providers were vacated—Audrey Edmunds in 2008, Kathy Henderson in 2012, Jennifer Del Prete in 2014, and Rene Bailey in 2014—based on the argument that a change in medical thinking over the past few years constituted “newly discovered evidence.”
This approach has been effective in righting past wrongs, but ironically, it will be less persuasive against recent convictions (like those of Cammie Kelly, Michelle Heale, and Joshua Burns, for example), since the debate has now been raging for a decade or more.
With the decision, the court released Fero from court supervision while she awaits the state’s response.
Like so many women in her position, Fero has received the support of her family and community through the years, and the decision in her favor noted:
Fero also submits several exhibits attesting to her positive influence on others while in prison. These are irrelevant to her petition to this court because they are not material to the conviction.
Press coverage quoted her attorney, J. Christopher Baird of Perkins Coie LLP in Seattle, who said, “Our client is a truly wonderful person, and it feels great to get the result we feel she deserves.”
If you are not familiar with the debate surrounding shaken baby syndrome, please see the home page of this blog.
Richard Britts and his daughters -courtesy of Richard Britts
Illinois father Richard Britts has been cleared of shaking accusations, two years after his younger daughter, three months old at the time, suffered a seizure while in his care. Jurors acquitted him earlier this month after hearing testimony from both prosecution doctors and forensic pathologist Dr. John Plunkett. The child seems to have fully recovered from the incident.
It’s the latest case calling into question “shaken baby syndrome” – a triad of symptoms that some doctors say can only be caused by violent shaking. Other doctors, however, say existing medical problems can cause the same symptoms, casting doubt on a diagnosis that has landed several people nationwide behind bars.
A Twin Case in Jersalem
A report in The Jersalem Post (“Israel’s best-selling English daily and most-read English website”) offers an unusual slant on a shaking diagnosis with this statement:
Shaken baby syndrome is an intermediate condition between an accident and physical abuse of children.
In the article’s focus case, a father is facing a manslaughter charge in the death of his 4-month-old son, who with his twin sister was rushed to the hospital in January with “internal injuries,” including bone fractures.
The news report explains the prosecution’s thinking:
The state said it will argue that the death was caused unintentionally, but that the father did intentionally commit acts of violence against the baby who died and that those acts of violence did cause the baby’s death, making an allegation of manslaughter appropriate.
A Successful Appeal
An appeals court in Florida has partially reversed a shaking conviction, ordering a new trial because the first judge had excluded biomechanical testimony. The published opinion focuses on what Florida law allows in the testimony of a biomechanics expert. The key paragraph opens:
Kieran Lloyd, who at 7 months eagerly provided data on repetitive bouncing motions by playing in a commercial jumping toy.
Florida courts have held that a biomechanics expert is not qualified to give a medical opinion regarding the extent of an injury. Stockwell v. Drake, 901 So. 2d 974, 976 (Fla. 4th DCA 2005); Mattek v. White, 695 So. 2d 942, 943 (Fla. 4th DCA 1997). However, it has been recognized that a biomechanics expert is qualified to offer an opinion as to causation if the mechanism of injury falls within the field of biomechanics. See Houghton v. Bond, 680 So. 2d 514, 521 (Fla. 1st DCA 1996) (holding that the defense’s biomechanics expert was qualified to testify that 90% of the plaintiff motorist’s injuries were caused by his hitting the dashboard as a result of his failure to wear a seatbelt because the expert was not offering a medical opinion based on brain anatomy and function); Behn v. State, 621 So. 2d 534, 536 (Fla. 1st DCA 1993) (recognizing that an expert in the field of biomechanics would be qualified to testify that a delay in an automobile accident would have altered the fatal consequences)..
The expert whose opinion was prohibited is biomechanic John Lloyd, PhD, whose most recent paper I described in this blog posting. The key paragraph of the opinion concludes:
In this case, Dr. Lloyd was not offering a medical opinion as to the extent of the victim’s brain injury, a matter which was not in dispute. Rather, based upon his biomechanical studies, he opined that (1) a child of the victim’s height and weight could have sustained similar brain injuries by falling out of a day bed; and (2) shaking alone could not have caused such injuries. We conclude Dr. Lloyd was qualified to offer these opinions as to causation because the mechanism of injury (falls and shaking) fell within the field of biomechanics
A Suicide Attempt
Finally, after a preliminary hearing that lasted four days, a California judge has ordered a foster father to stand trial for murder and child abuse in an especially murky case. The defendant called 911 in November of 2010 with a report that a baby was choking on milk. During interrogation later he said he had accidentally knocked the child from the table in his bouncy chair.
Vacaville Reporter Ryan Chalk summarized the medical testimony in a news story, no longer on line, in The Reporter:
Wednesday saw the conclusion of testimony from Dr. Michelle Jorden, a forensic neuropathologist.
Jorden testified that it was her opinion that Buddy had suffered a traumatic brain injury leading up to his choking episode.
“I think it’s a combination of shaking and impact,” Jorden testified as to the cause of the injuries.
And from another day’s coverage:
Dr. Rachel Gilgoff, a child abuse pediatrician, testified that “both sides of his brain were extremely compromised,” as tests revealed he was suffering from significant bleeding and swelling in the brain.
“His injury is extremely consistent with abusive head trauma, or shaken baby syndrome,” Gilgoff testified.
I’m guessing there was no evidence of impact, because there’s none mentioned in the articles.
The defendant, Reginald Tanubagijo, attempted suicide at some point before the preliminary hearing, according to The Reporter:
Tanubagijo had already been arrested and released on bail, and during that time, Officer Michael Shephard responded to the Tanubagijo home for a report of a suicide attempt.
Shephard testified that he found Tanubagijo slumped over with a bloody towel over his arm and a very large laceration to his wrist.
Inside the kitchen, Shephard testified that he found a note that read, “I killed Buddy.”
Other notes found at the home read, “I did killed Buddy,” and “Tell the judge I did killed Buddy,” the officer further testified.
The child’s biological mother has filed a civil lawsuit charging negligence by the county and others who allowed the defendant to be a foster parent, the most recent coverage reports.
It’s too early to celebrate, but the Sacramento Bee reports that Governor Jerry Brown is expected to pardon Shirley Ree Smith, the grandmother whose conviction in a shaking case was recently reaffirmed by the Supreme Court:







 Instead of reconsidering their model, however, proponents of shaking theory “took a course I never imagined they would be able to take, claiming there never was a triad,” Papetti marveled in our interview. In his book, he noted that changing the name of the diagnosis from “shaken baby syndrome” to “abusive head trauma” did not address the fundamental problem that the entire theory was speculation. “It merely changed the diagnosis’ name for legal purposes.”
Instead of reconsidering their model, however, proponents of shaking theory “took a course I never imagined they would be able to take, claiming there never was a triad,” Papetti marveled in our interview. In his book, he noted that changing the name of the diagnosis from “shaken baby syndrome” to “abusive head trauma” did not address the fundamental problem that the entire theory was speculation. “It merely changed the diagnosis’ name for legal purposes.”







 This quote illustrates the kind of rhetorical thinking that can obscure logic when the topic is child abuse. Despite the implications of the phrase “paid reports from defense medical experts,” the state’s doctors are also paid for the time they spend preparing reports. The objection, then, must rest on who is paying, as if the opinions of the state’s doctors should necessarily prevail over the opinions of the defense experts. And I wonder whether the pediatricians have really thought through the question of “independence.” The medical examiner’s office is ordinarily on the same team as the detectives and the prosecutors, all agents of the state. In child abuse cases, the diagnosing pediatricians are also part of the prosecution team. In three instances in less than two years now, individual examiners have concluded that medical factors identified by defense doctors could have explained the infant deaths, putting the examiners at odds with physicians who are usually their allies. To me, that sounds like the essence of independent thinking.
This quote illustrates the kind of rhetorical thinking that can obscure logic when the topic is child abuse. Despite the implications of the phrase “paid reports from defense medical experts,” the state’s doctors are also paid for the time they spend preparing reports. The objection, then, must rest on who is paying, as if the opinions of the state’s doctors should necessarily prevail over the opinions of the defense experts. And I wonder whether the pediatricians have really thought through the question of “independence.” The medical examiner’s office is ordinarily on the same team as the detectives and the prosecutors, all agents of the state. In child abuse cases, the diagnosing pediatricians are also part of the prosecution team. In three instances in less than two years now, individual examiners have concluded that medical factors identified by defense doctors could have explained the infant deaths, putting the examiners at odds with physicians who are usually their allies. To me, that sounds like the essence of independent thinking.







